An aortic dissection is a life-threatening condition. With prompt treatment and ongoing management outcomes greatly improve. Management is dependent on factors such as the severity and location of the dissection. On this page management strategies at each stage of the treatment process will be discussed.
Pre-operative Management
|
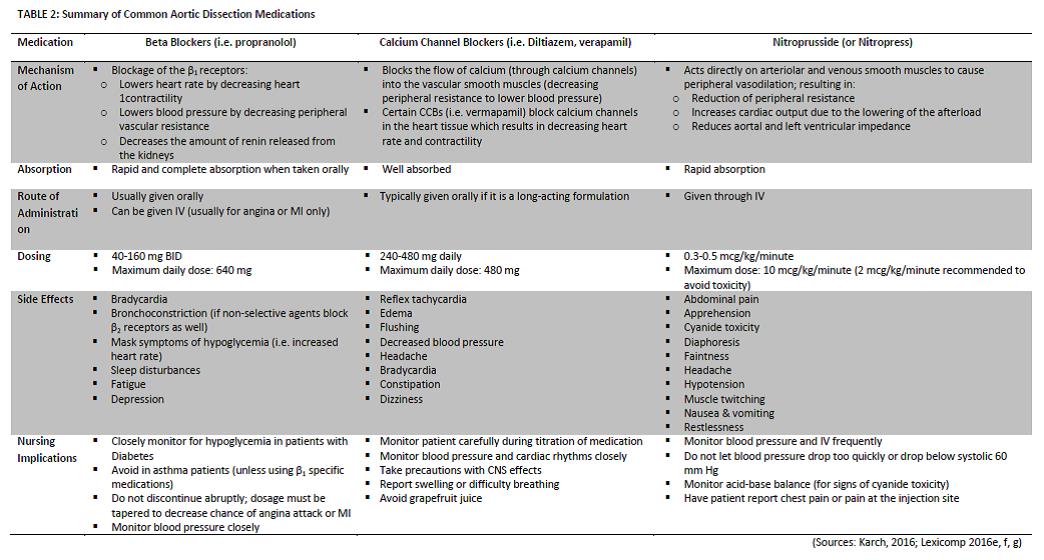
Once a diagnosis of an aortic dissection is confirmed, there are various interventions that nurses can implement to improve the comfort of the patient while they wait for surgery. The main priority is to decrease the chance of the dissection worsening (Ince & Nienaber, 2007). This is of particular concern in Type A dissections, which are considered a medical emergency. Pharmacological interventions are most often used to minimize this risk. Medications are given to lower the blood pressure to a target of a systolic blood pressure between 100-120 mm Hg and to lower the heart rate to below 60 beats per minute. The rationale behind this is to decrease the stress being placed on the tear with each heartbeat. Typical drugs given are beta blockers, calcium channel blockers (for those who are intolerant of beta blockers), nitroprusside, or a combination of these (Mousa et al., 2015; Huang et al., 2012). Blood pressure should be monitored closely throughout the pre-operative stage to assess the effectiveness of these interventions. For more information on medical management, see the Common Medications for the Management of an Aortic Dissection section (Table 2).
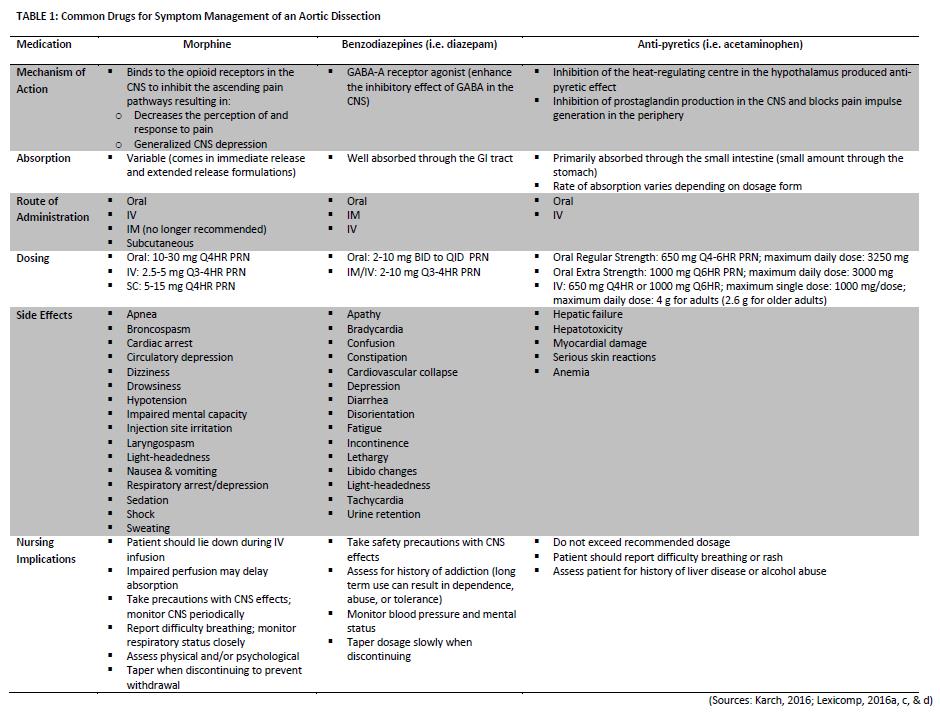
Individuals with a dissected aorta will typically present with sudden onset pain, anxiety or feelings of impending doom, and fever (Khan, 2001). Once blood pressure and heart rate are controlled within the target range, the next priority is symptom management, in particular pain management. Physical stress (from pain or fever) and emotional stress both result in the release of the steroid hormone cortisol which causes an increase in blood pressure (McCance, Huether & Brashers, 2014). Therefore, it is important that these symptoms are treated promptly. Medication are the most common intervention utilized in symptom management (See Table 1). The nurse can also implement non-pharmacological measures to treat these symptoms. These can include: hot/cold therapy for pain, cold compress for fever, psychological treatments for pain and anxiety (i.e. deep breathing), etc. (Potter & Perry, 2014). |
Intra-operative Management

|
Surgical repair of the damaged aorta is usually the first line of therapy for most people with an aortic dissection (Castrovinci et al., 2016). However, different procedures are performed to treat type A (tear in the ascending aorta) versus type B (tear in the descending aorta) dissections.

FIGURE 1: Example of a reconstructed aorta following a Type A dissection (Source: http://www.lenoxhillheartvascular.com/Aortic-Conditions.html)
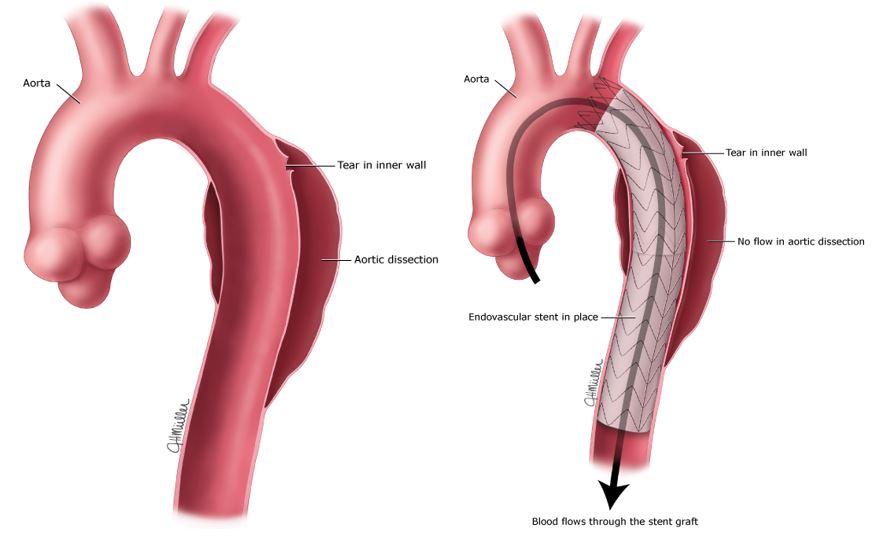
FIGURE 2: Aortic dissection prior to surgery (right); Aorta following the placement of an endovascular stent to prevent blood flowing through the tear (left) (Source: http://goo.gl/jBftMS)
|
Post-operative Management
|
Immediately following any surgical procedure, the nurse has various roles. Many of these include periodic assessments of the systems and pain (Lewis, et al., 2014). This is to establish a baseline immediately following surgery and for prompt identification of complications. Pain is also a major part of post-operative care and should be assessed periodically and treated as required. In the case of a post-aortic dissection patient, particular attention should be paid to the cardiac assessment for any signs of complications.
Patient education is also an important part of the nursing management of aortic dissection. Further details of patient education are provided on the patient resources section of this site. |
Common Medications
|
As noted above, the main goal of pharmacological interventions for individuals with aortic dissection is to lower the blood pressure and heart rate (Ince & Nienaber, 2007). This will decrease the stress exerted on the aortic wall and decrease the risk of the tear worsening. Ideally, systolic blood pressure should be maintained between 100-120 mm Hg and the heart rate decreased to <60 beats per minute. The following table summarizes some of the common drugs used to achieve these ranges in aortic dissection patients.
|