PathologyWhat is it?An aortic dissection is a tear in the intima of the aorta, the thin inner layer of the arterial wall, resulting in the degeneration of the medial layer of the aortic wall. Consequently, blood flow is diverted through the tear into the media creating a false lumen.

|
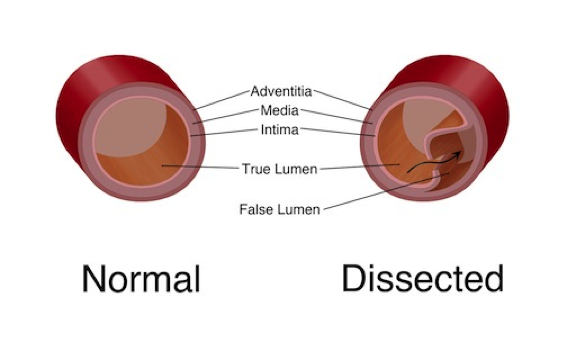
FIGURE 1: Normal structure of the aortic wall (left) vs. Dissected aorta with a false lumen (right) (Source: m.ufhealth.org)
As the dissection increases, the blood flowing through the false lumen occludes blood flow through the true lumen of the aorta, effectively cutting off systemic circulation to aortic branches (the coronary, brachiocephalic, intercostal, renal, and iliac vessels) (Nathan, Xu & Gorman, 2011).
A dissection can occur at any point along the aorta. Most tears originate just above the sinotubular junction or distal to the left subclavian artery (Nathan, et al., 2011).
|
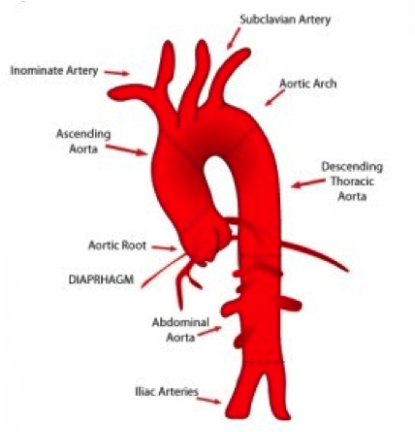
FIGURE 2: Branches of the aorta (Source: www.aorticdissection.co.uk)
|
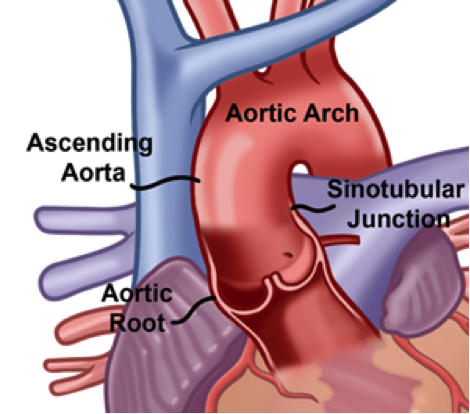
FIGURE 3: Sinotubular junciton, a common site for aortic dissection, is a region located between the aortic valve and the beginning of the aorta (Source: valleyheartandvascular.com)
|
|
From the initial site there is a retrograde and/or antegrade extension of the dissection which can lead to aortic incompetence by separating the aortic root from the aortic valve. Occlusion of the blood vessels results in end-organ ischemia. This occlusion can be caused by both static narrowing and/or dynamic compression. Static narrowing is the intersection of the line of dissection and the vessel origin where a hematoma has formed in the vessel wall resulting in stenosis or occlusion of the side-branch (Hiratzka, Bakris & Beckman, 2010). Dynamic compression is the result of the dissection flap being on the opposite side of the branch-origin causing occlusion during diastole when the true lumen collapses and the intimal flap closes over the opening to the branch vessel (Figure 4B). This occlusion is corrected during systole (Figure 4A) (Hiratzka et al., 2010).
|
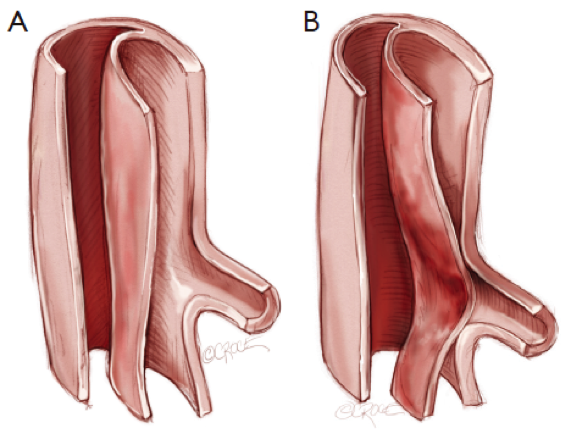
FIGURE 4: Dynamic Compression (Source: www.annalscts.com)
|
Classification
|
The most common classification of aortic dissections is the Stanford system which classifies dissection class based upon the area of the aorta impacted. Any dissection involving the ascending aorta, regardless of site of origin, is a class A dissection. Class B is any dissection not involving the ascending aorta (Crawford, Svensson & Coselli, 1989).

|

FIGURE 5: Classification of an aortic dissection by
the region affected (Source: www.radiologyassistant.nl) |
Aortic Dissections from fairmanstudios on Vimeo.
Etiology
Any condition that results in a weakening of the media of the aorta creates a physical predisposition for aortic dissection. These conditions include genetic conditions such as Marfan’s and Ehlers-Danlos syndrome. Additionally, any condition which results in dilation of the aorta, including atherosclerosis and non-specific connective tissue disease (specifically affecting the bicuspid aortic valve), can lead to aortic dissection. Cardiac interventions including surgery can increase the chance of a dissection as well, though this is very rare (Jonker, Schlosser & Indes, 2010).
Epidemiology
Aortic dissection affects approximately 0.5 – 2.95 persons per 100,000 each year worldwide (Hagan et al., 2000). In the United States, there are approximately 3 – 4 new cases per 100,000 persons each year, with an incidence of approximately 2,000 persons (Olsson, Thelin, Stahle, Ekbom & Granath. 2006). Hagan et al. (2000) report that overall mortality for both type A and B dissections is approximately 27%. Mortality broken down by classification is below:

Post hospitalization, the 10 year survival rate is estimated to be between 30 and 60% (Braverman, 2010).
Exact numbers for Canada are more difficult to ascertain as Statistics Canada includes aortic aneurysms with aortic dissection in mortality tables. 3.4 persons per 100,000 died as a result of aortic dysfunction in Canada in 2009 (Statistics Canada, 2012).
Exact numbers for Canada are more difficult to ascertain as Statistics Canada includes aortic aneurysms with aortic dissection in mortality tables. 3.4 persons per 100,000 died as a result of aortic dysfunction in Canada in 2009 (Statistics Canada, 2012).
Developmental Considerations
|
Increased age is associated with an increased incidence of aortic dissection. Over 70% of patients diagnosed are over 60 years of age. Twenty-seven percent of patients diagnosed are between the ages of 17 – 59. Individuals over 40 typically have concurrent diagnoses of hypertension or atherosclerosis whereas individuals under 40 tend to present with Marfan’s syndrome, bicuspid aortic valve, or iatrogenic factors such as a previous aortic intervention. Gender is also a strong factor with an incidence ratio of 3:1 males to females (Thrumurthy et al., 2011).
Developmental patterns in Canada are consistent with those in the US and UK with a strong association between increased age and incidence, and persons impacted being 70% male. Males over 50 are the most affected group in Canada (Statistics Canada, 2012). |

FIGURE 6: Actor John Ritter, who died at age 54, is an example of the patient population most susceptible to aortic dissection (Source: https://goo.gl/Ii3pZ5)
|
