Watch this video by the Cleveland Clinic for a great explanation of Aortic Dissections! (SOURCE: https://goo.gl/6knKFg)
|
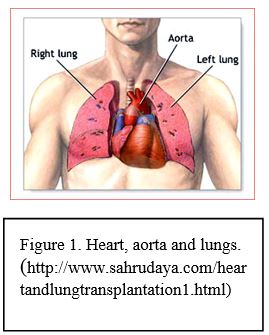
PathologyThe aorta is one of the most important blood vessels in the human body. Blood oxygenated by the lungs is pumped through the heart. From the heart, blood travels through the aorta to be distributed through the entire body (see figure 1) (McCance, Huether, Brashers & Rote, 2014).
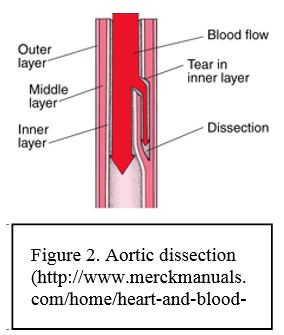
Aortic dissection occurs when there is a tear in the inner layer of wall of the aorta and blood enters the wall of the artery (McCance, Huether, Brashers, & Rote, 2014) This blood pushes through the tear separating (dissecting) the middle layer of the wall from the outer layer and creating a false channel (lumen) within the wall of the aorta (see figure 2) (Hallett, 2016; Nienaber & Clough, 2015). Tears in the aorta, which happen closer to the heart (in the ascending aorta) are classified as Type A and tears which happen in other parts of the aorta are classified as Type B (Nienaber & Clough, 2015). |
Risk FactorsLong-term high blood pressure is the most important risk factor for aortic dissection (Ince & Nienaber, 2007). In addition atherosclerosis and previous cardiac surgery can increase the risk for aortic dissection (Ince & Nienaber, 2007). Some genetic conditions can also increase the risk of aortic dissection including Marfan’s syndrome, Turner’s syndrome and type 4 Ehlers-Danlos syndrome (Nienaber & Clough, 2015). Genetic causes of aortic dissection are more common in people less than 40 years of age (Ince & Nienaber, 2007; Nienaber & Clough, 2015). Smoking, direct blunt trauma and drugs (cocaine and amphetamines) are also risk factors (Nienaber & Clough, 2015).
|
|
ManifestationsThe most common system of aortic dissection is sudden onset severe chest or back pain (Nienaber & Cloug, 2015). Other symptoms include dizziness, loss of consciousness or paralysis of the legs (Nienaber & Cloug, 2015). Aortic dissection can lead to heart and kidney failure and death (BMJ Publishing Group Limited, 2016).
|
ManagementType A aortic dissections are emergencies and require immediate surgery to be repaired (Ince and Nienaber, 2007; McCance, Huether, Brashers, & Rote, 2014). Type B aortic dissections can be treated with medications to lower blood pressure and decrease the force of blood pumped out of the heart, however may sometimes also require surgery (Ince and Nienaber, 2007). After leaving the hospital medications to lower blood pressure and decrease the force of heart contraction will be prescribed (Ince & Nienaber, 2007). In addition imaging and clinical assessments will be performed at regular hospital visits (Ince & Nienaber, 2007).
|
For more information visit The John Ritter Foundation for Aortic Health at http://johnritterfoundation.org/
Specific Patient Education for Nurses
Nurses should emphasize to patients the importance of the proper management of hypertension, as it is the most important risk factor for aortic dissection (Ince & Nienaber, 2007). In addition, nurses should stress the importance of seeking prompt medical attention should patients experience sudden onset chest or upper back pain (Khan, 2001). Patient education is vital following a diagnosis and/or surgical intervention for an aortic dissection. For the best outcomes, patients will continue to take antihypertensives for the remainder of their lives (Ince & Nienaber, 2007). Patients are also encouraged to control their blood pressure through other means. This can include lifestyle modifications such as dietary changes (i.e. low sodium diet), smoking cessation, and light physical activity (Heart & Stroke Foundation, 2013; Heart & Stroke Foundation, 2014; Chaddha et al., 2014). Heavy physical activity is not recommended due to the stress the exertion puts on the aortic wall (Chaddha et al., 2014). Furthermore, regular MRI or CT scans will be required to monitor the dissection for growth or worsening (Ince & Nienaber, 2007).
